Equipment and infrastructure refer to fixed assets on the balance sheet. Equipment is relatively movable, while infrastructure is fixed and virtually inseparable from physical facilities—buildings, electrical networks, water and sewer systems, etc.
When a donor initially expresses a desire to fund "a piece of equipment, something physical, to ensure that the money is not wasted," they do not realise that the opposite is often true. The following paragraphs explain how this contrary reality is invisible to donors.
When considering used equipment, the following questions must first be asked: What is the remaining useful life of the equipment? Can it still be repaired and maintained? Why do Canadian hospitals no longer want it? If the answers to these questions are satisfactory, the next questions are similar to those asked when purchasing new equipment.
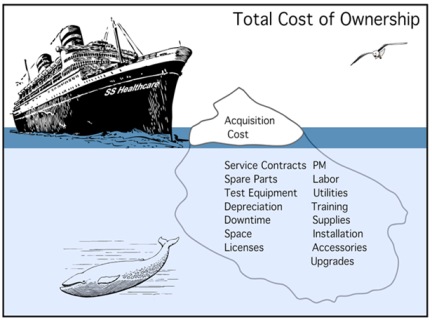
The hospital invests in new equipment and infrastructure with great caution, as the initial investment is only the tip of the "cost iceberg": the submerged part will generate an increase in recurring costs for staff, training, operation, maintenance, etc., to prevent premature obsolescence of the equipment or infrastructure.
Added to this is the difficulty of coordinating equipment donations from various sources and liaising with donors who have strict priorities.
Accepting a donation of equipment entails invisible costs (to the donor) that are often unsustainable for the recipient. In a context of very limited resources, the cost of installing and maintaining technological equipment consumes a significant proportion of the discretionary budget (which is very limited in Uganda) and, as a result, significantly reduces the budget available for "everything else." It should also be noted that several countries, including Uganda, impose customs duties on equipment entering the country even if it is donated—a measure that ensures that donations do not undermine the market for local medical equipment representatives and that the country is not flooded with obsolete equipment.
According to the World Health Organisation (WHO), up to 60% of the medical equipment in a non-profit hospital in sub-Saharan Africa may have been donated (new or used) from abroad. However, up to 60% of all this equipment has stopped working within six months of entering the country; some has never even worked. This situation illustrates the imbalance between power, perceived priorities and the desire to show off the "tangible gift" sent to Africa.
According to the WHO, in high-income countries, less than 1% of hospital equipment is defective and non-functional; in Africa, the figure is over 50%.
Finally, the acceptance of multiple donations means that a recipient, such as a hospital, may end up with several models and brands of the same device, which causes training and maintenance costs to skyrocket.

